The Use of CBCT in Endodontics: Intraoperative Scans
Today’s blog will focus on the use of CBCT technology to aid in detecting root canal anatomy during the course of endodontic therapy.
Customarily, our office will use CBCT technology to aid with our pre-operative diagnosis and treatment planning. The three dimensional rendering can elevate our ability to detect endodontic pathology, enhance the visualization of the peri-radicular bone and better ascertain the extent of resorptive defects. Overall, the use of CBCT technology in our endodontic practice has been a game changer in our ability to visualize and analyze the root canal system. Today’s case is a good example of a case where I utilized the CBCT scan to help locate a deep canal split in the distal root and a mesial buccal canal that had constricted in the coronal third of the root.
A 54 year old female patient presented to our office last month with a report of acute discomfort localized to tooth #30. An all ceramic restoration was placed three months prior. Since that time, a strong sensitivity to cold had developed in conjunction with slight chewing tenderness. I examined the tooth clinically and confirmed an acute irreversible pulpitis localized to the first molar. After discussing the treatment options we decided to move forward with endodontic therapy. On the pre-operative radiograph the canal system appeared to be rather straight forward with some slight coronal calcification of the mesial canal system. Overall, I was not too concerned with the pre-operative anatomical configuration. Once inside the access, both the mesial lingual and distal buccal canals were located. After troughing with an ultrasonic tip under high magnification, I could see the delineation of reparative dentin over the orifice of the MB canal. A slight stick with a 6 C plus file was noted along the lingual wall of the distal canal; however a separate orifice could not be visualized under the microscope.
Instead of continuing to trough down the root with an ultrasonic tip or Munce bur, I opted to take an intra-operative CBCT scan with CAOH to provide an accurate road map of where the canals were located. Placing CAOH is helpful as the radio-opacity of the material can be used as a reference point. Additionally the CBCT scan has a ruler function indicates exactly how many millimeters further I need to navigate down the root. Using the scan prevents the unnecessary removal of radicular dentin and facilitates locating the canals.
I have included several different slices from the scan below:
Axial Slice in the apical third of the root suggesting the presence of separate portals of exit for each canal.

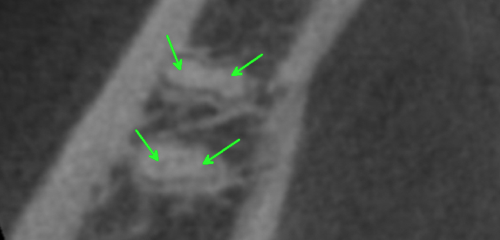
Distal Root, Coronal View, Arrow indicating the lingual split .

Mesial Root, Coronal View, Arrow on CAOH placed at apical extent of trough, indicating that my path was centered within the canal and “on target” to locate the orifice.
With the information from the scan I was able to determine exactly how far I needed to progress in order to find each canal. I could also confirm, in three dimensions, that I was centered within the mesial buccal canal path and “on target” to find the canal. CBCT technology is an incredible innovation for the field of endodontics. We are finding that a three dimensional rendering can elevate the degree of care not only with pre-operative diagnostics but also with intera-operative treatment. The final radiograph can be seen below with four separate portals of exit for the four canals. Stay tuned for more blogs on the use of CBCT in endodontics.

Post Operative Radiograph

Pre Operative Radiograph
Thanks for visiting Tri-City and Fallbrook Micro Endodontics of San Diego, CA.